
It was so unusual that I wanted to write it up and send it to a journal for publication. But I didn't want to embarrass my colleague, who was a good guy. So I tell the story here for the first time.
When something shows up on a mammogram that warrants investigation, but can't be felt, you need to sample it using some form of Xray guidance. (If you can feel it, you can poke a needle into it in about two seconds, taking a sample for analysis. Or do a surgical biopsy. But when you can't feel it, there's no simple way to get at it in the office.) There are two main choices: wire localization, or sterotactic biopsy. In the former, the radiologist guides a wire to the area, and the surgeon then operates, following the wire to the target. In the latter, the radiologist does the whole procedure, with the woman lying prone, breast hanging down into a device which is aimed by Xray and then sends a biopsy-needle to the zone. There are, as usual, pros and cons of either method. Choosing one over the other depends on factors I might get around to some day. More and more, the stereotactic method is used; which is fine. In an ideal world, however, there'd be surgical input into the decision: coordinating diagnostic interventions in breast disease can eliminate a lot of unnecessary or duplicated testing. But I digress...
Marlene had had needle localization for a shadow on her mammogram. "Enormous" would be the word to describe the organ in which the shadow resided. The surgeon who did the procedure -- struggling, I'd imagine, in a very deep hole, following a flimsy wire into oblivion -- unfortunately cut the wire as he was working his way to the far end. As one might expect, gravity being what it is, the wire disappeared into the abyss. The surgeon spent a very long time trying to locate it and the target to which it pointed, and failed. He even transferred her from the surgicenter to the hospital across the street, where he used a mobile Xray machine (called a C-arm, for the shape of the business end which can be positioned to take live-action pictures on an operating table) without success. He gave up. Fully recovered and not a little pissed, Marlene came to see me for a second opinion.
Reviewing the Xrays led me to a couple of conclusions. First, uncomfortably: the shadow in question had, comparing mammograms taken regularly for several years, quite innocent characteristics (maybe fodder for another post, sometime) and -- more importantly -- had been unchanged for at least eight years. I, in other words, wouldn't have recommended biopsy in the first place. Second, the surgeon had given a pretty thorough effort to finding the wire, and I had no reason to think I'd be any more successful. We deliberately leave metal objects of all sorts in people; I didn't think the wire was in need of removal for its own sake. So I recommended watchful waiting, beginning with a repeat mammogram in a few months. If anything, Marlene seemed relieved. She's had enough plowing around in her breast for a while, thanks very much. She might have been a teensy bit annoyed at having undergone what may have been an unnecessary procedure, but we didn't dwell on that aspect. So when she reappeared in my office later, as planned, bearing the repeat Xray, we were both pleased to note that the shadow remained quite benign-appearing and absolutely stable. I was, however, a little puzzled to note that the wire was no longer there.
As usual, there are several types of wires from which to choose. Below is the kind I like:
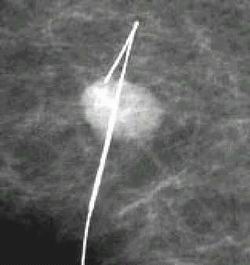
It has a sharp backwards bend at the end, which discourages accidental dislodgment -- as can happen during the hubbub of transferring from the radiology area to the OR (not rarely involving a ride in a car) or during the operation itself. It also -- not relevant to the present tale, but giving credit to the inventor -- has a change in diameter near the end, which is helpful in pointing out that you're nearing the target as you dissect. It hadn't occurred to me until now (why would it have? It had never come up) that the characteristics of the hook could, with motion of the breast, allow for inching it forward. Guessing the wire had migrated itself to the periphery of the breast, outside the mammogram field, I ordered a regular chest Xray, and indeed it showed the wire. But not hardly where I'd expected it. Not hardly at all.
At the far edge of her right lung, is where it was. It had originally been in her left breast! And -- for you anatomists out there -- subsequent views showed it was definitely within the lung, not overlying it on the outside. Now, here's the hard part, because I'm not clever enough to be able to draw explanatory pictures and load them into this blog: the only way this could have happened is if the wire had humped itself directly down through the breast, through the chest wall, and into Marlene's heart: her right ventricle, to be precise, after which it was flushed out into the pulmonary artery and sent into the lung. The only other avenue was for the wire to have entered a vein in Marlene's breast -- or the big vein under her collarbone (the subclavian vein) and then gone to the heart. But the wire was at least two inches long. No way it could have made the twists and turns required of that circuit, starting its journey through a small vein.
"I've got some good news, and some bad news," I told Marlene. "The good news is that the shadow in your breast continues to look harmless, and safe to leave alone. The bad news is that the wire..... DRILLED A HOLE THROUGH YOUR FRIGGIN' HEART, PASSED RIGHT THROUGH IT AND STABBED ITSELF INTO YOUR LUNG. YOU'RE GONNA DIE!!!!!" OK, I didn't say that last part. But I figured that's what she'd hear, no matter what I said. Who wouldn't? I explained as mildly and as carefully as I could, drawing the sort of pictures I'd be doing now if I were clever enough, pointing out that if anything bad might happen, it'd already have occurred. I must have done alright, because Marlene remained seated calmly, as opposed to falling to the floor. I told her honestly that I'd neither seen nor heard of anything like it, and that I'd get consultations from cardiologists and chest surgeons; but that I thought the wire had done all the traveling it would ever do, and had come peacefully to rest where it would do no further harm. She liked that.
Catheter-wielding cardiologists and scalpel-wielding heart surgeons agreed: leave the damn thing alone. More damage was possible from trying to get it out than it could conceivably cause left in place. Subsequent Xrays over the next year confirmed it was happy where it was, and so was she. I'm pleased to say I'd never cut and lost a wire in a breast; but after meeting Marlene, I was even more careful with them than I'd been.




{kind=link}
15 comments:
Absolutely amazing....
Wow! How is it that the wire could have done that without causing any apparent problems? That *is* pretty amazing.
By the way, I like your title.
OMG!!! Am I right in concluding that she could have suffered cardiac tamponade and... (you know what)?
Wow...So what happened long term? Did she live long and have no problems ever, from it being there?
Its feels really weird that I am reading this today. While my chest is sore and hurting from a "bone marrow aspiration" out of my sternum yesterday, with no sedation. I swear reading this story brought back the pains of him screwing that friggin tool into my chest and pulling back on the plunger. I wanted to move away from him, but I was afraid the needle would break or something...
How odd it feels to have just experienced that and then come here and read this? Its a small world Doc.!
Did fine, no further problems.
Holy Chuck Berry, father of Frog. *shudder*
Y'know, the only incident I've ever seen of a wire migrating was post-angio, when I assessed a patient who'd been normal in the ICU for two days and heard "lub-squeeeek! lub-squeeek!" for a heart sound. Turns out about an inch of angiocath guide wire had broken off and migrated into a heart valve.
That damn near gave me a nervous breakdown; if I'd'a been the nurse or MD dealing with a patient whose wire had gone on the anatomical equivalent of a Route 66 tour, I'd'a died.
Ever proof of how amazing the human body really is.
I guess there are no MRIs in her future...that would surely hurt on its way back out via magnet...
I wonder if she sets the metal detectors off in the airport?
"No, office, I have a wire in my lung, honest!"
I sometimes wonder about the necessity of mammograms, and think it's a trick to get people to part with their money.
It certainly seems called for on well-endowed women, but is it required for everyone?
My wife is small chested - 34A - and her doctor orders a mammogram for her annually. I ask how they can possibly do it, and my wife says it is extremely painful and the person pushes and pulls to try to get enough skin etc to squeeze between the plates. Doesn't sound justifiable to me, as her breasts are so small that surely anything would be obvious to a manual exam or a chest xray.
Not saying all doctors are like that, but they are in short supply here so maybe she does this to pad her income.
BTW, when I was a kid my neighbour's father died of breast cancer - he was 42. How is breast cancer detected in men??
Dr. Schwab ... that was incredible. You sure little gremlins didn't move that wire when you guys weren't looking? ;o)
Mark: in men, it's virtually always detected on physical exam, or by the person who has it: a lump. Mammograms aren't useful for screening men, nor do they give useful info when there's a lump in a man.
You're wrong about mammograms in small-breasted women. I agree it can be difficult. But the best way mammograms find the most early and practically 100% curable cancer is when they detect certain tiny calcium deposits. Those can't be felt on exam, and they don't show on a chest Xray.
But the best way mammograms find the most early and practically 100% curable cancer is when they detect certain tiny calcium deposits
Well, the problem is some of these tumors would never have progressed if remained undetected - ever heard of "overdiagnosis"?
And some tumors are so aggressive that they are going to kill you no matter when they are discovered. But if these very aggressive tumors are discovered earlier you have longer period of "being sick" before death.
Yet other tumors progress sufficiently slow that they are still curable when detected later.
Mammograms save lives only when they detect a small subgroup of tumors: those which are destined to progress before they are discovered but caught by mammograms before that. There are still disagreements as to how big this subgroup is.
Doctors love to use meaningless statistics like "30% mortality reduction" but this is a relative number based on your chance to die of breast cancer. Better statistics is number needed to screen to save one life. According to the USPSTF, one needs to screen 1200 women in their 50s for 10 years or 1700 40-something women for 10 years to save one life. During the same 10 years of yearly mammograms there is over 50% chance of having at least one false positive - some of which just for diagnostic mammograms but some fraction involves biopsies which as this article showed has some risk. There is also a chance of overdiagnosis -being treated for a small leision that would have never threatened one's life if remained undetected.
So there is a price to pay for less than 1 in 1000 (after 10 yearly mammograms) chance of having one's life saved. Is it worth it? Surely it is up to each individual woman to decide?
Back in the 1940s I read of a woman who kept laddering the nylon stocking on one leg, always in the same place. It was found that the point of a small sewing needle was just on the surface of the skin in her calf, the rest of the needle being in her leg.
Eventually she remembered an accident she'd had as a little girl, when a needle had gone into the palm of her hand on the opposite side of her body and disappeared. As intelinurse2b says, the human body is truly amazing.
It was recently discovered when my family doctor FINALLY decided to x-ray my right leg, which had been swollen and in pain for years, that wire was in my right thigh--left over from a heart cath three years earlier. No doctor wants to discuss it. If I am on my feet just doing housework, the next day I have to be off of it cause it is so swollen I cannot even put my shoe on. Any ideas on what I do? Go back to the guy who left it there? HELP!@!!
Seeing the person who left it there would seem a logical place to start.
Post a Comment