Thursday, August 27, 2009
Toons
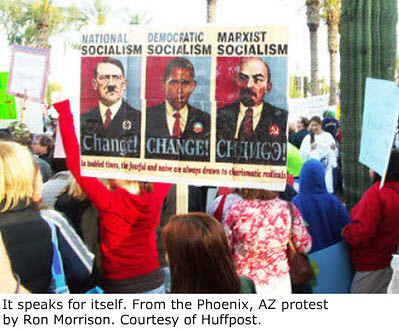
In a comment on my previous post, a series of slides is recommended. I like the cartoon above even better. In simplicity there can be great truths.
Wednesday, August 26, 2009
Retort

Sooner or later, in any discussion of health care reform (to the extent that screaming and fear-mongering can be gotten past and actual thoughts exchanged), the issue of tort reform is raised. On that subject I'm of two or more minds. Neither a student of the various proposals nor particularly well-versed on the veracity of claims and counter claims about tortophobia adding to costs of medical care, I can only speak based on personal experience. Which is why I'm multi-minded. I've seen good and bad. I don't think I altered my practice style to avoid malpractice suits, but I can see why people would.
The central issue is this: there's a difference between malpractice and adverse outcomes. Most certainly, the one leads to the other; but the other does not imply the one. Were that distinction properly made and encoded in the law, the rest of the issue would become moot. If malpractice suits were about bad care -- actual errors, poorly thought-out diagnoses or treatments, willful neglect of patient needs; that sort of stuff -- I'd have no problem with them.
I was raised among lawyers. I've lived in their dens, eaten their food, learned their language. I agree with their claim that malpractice suits have, over the years, led to improvement in care, institution of protective procedures. And I absolutely agree there are bad doctors out there; lazy, lacking in judgment, in it for the money. Drinkers, drug users. Representing an overwhelmingly small minority, they nevertheless give us all a bad name; they are the cause of and the justification for the worst views the public has of us.
But, unlike the guy struggling to fix my freezer as I sit and type this (peering occasionally at what he's doing: my home improvement skills have largely osmosed from such viewings), I dealt with soft stuff. Every freezer of this type is exactly the same; the wires, the machinery, the outcome if you plug x into y. Not so of us humanoids. (I'm not saying what he does is less important; we're having to get along without freezing tonic cubes for our G and T's [a trick I highly recommend to anyone so inclined]. Or, judging by his grunts and mutterings, any easier. Just more predictable.) If he makes the correct diagnosis and replaces the parts properly, the outcome is the same for the same problem, over and again, on every like freezer. I've had some sub-optimal outcomes, despite (take my word for it, okay?) doing everything right. Not often. Not, thankfully, catastrophic. But the possibility is always there.
I've been sued, and I've written about it. It's humiliating, frustrating, depressing, and anger-inducing. I'd say that's entirely because of my certainty that in no case was malpractice, as I understand the term, committed. On the other hand, had I ever done something (or failed to do something) in a way that fell into that category, the last thing I'd want to do would try to defend it on a witness stand, nor try to prevent the patient from being compensated. Patients need a mechanism by which they can be protected from errors, and their injuries redressed. What form that takes is a complicated subject. The current system, because it fails to separate bad outcome from errors in management, isn't the proper mechanism. It wasn't my intent, in writing this, to suggest solutions.
My point, at last, is that I don't think tort reform, per se, will have much impact on the total cost of health care. Reducing errors will. Addressing inefficiencies and variations in treatments among doctors will. To the extent that docs order tests to cover their legal asses, such behavior would be reduced, asses covered, if there were guidelines that indicated when such tests were medically necessary and when not. It's true that there were times, when deciding a course of action based on clinical judgment alone (diagnosing appendicitis without a CT scan or ultrasound is a perfect example; taking a patient with a rigid abdomen to the operating room without the delay of additional testing is another), that I felt a slight breeze on my backside. Many docs are unwilling to do it; partly out of fear, but partly, also, out of being trained in the era of judgment coming in pixels. I guess you can't legislate judgment, but guidelines would help.
And yet it seems there's no discussing it without raising the specter of rationing and death panels. When President Obama suggests that investigating what works would save lots of money and improve care, he's exactly right. That's where the big bucks are spent, and wasted. Addressing it would solve much, including the need for tort reform.
The political party who has argued for reducing Medicare since it began, whose most recent candidate ran on cutting it, has now, for pale political reasons, resorted to demagoging attempts to do just that, as fascist terror. Without diminishing service at all, huge amounts of money could be saved by doing exactly what Obama proposes. Surely there are a couple of Republican senators and representatives who know this. But, clearly, the resistance is not about effective reform. It's about politics, and defeating the party in power.
The public be damned.
Tuesday, August 25, 2009
Grand Old Times

Nice Grand Rounds up over at the resurrected Dr Charles. His balloon is on the rise again, even as the hot air leaks soundlessly out of mine. Dr Charles has always been one of the most lyrical of medical bloggers, and it's nice that he's rediscovered his muse.
Friday, August 21, 2009
Stupid

Uuggggghhhhh.
Sorry.
I feel dirty, I need a shower, I may have to kill myself. Where are the death panels when you need them?
So Jon Stewart interviewed Betsy McCaughey last night, on The Daily Show. She's the one credited with raising alarms about the dastardly implications in the health care bill regarding end of life counseling. "Death panels," evidently, wasn't her exact term. "Disgusting," is what she said she wrote in the margins when reading it.
There was a point to which she kept returning (in between quite amazing dramatic gestures to the audience -- the kind when a stand-up comedian goes, "Am I right? Am I right? Huh? Huh?"). Medicare reimbursement is increasingly tied to performance standards, and it's an issue about which I've written a bit, and which, in its execution, is potentially problematic for all doctors. Nevertheless, her interpretation regarding end of life counseling was utterly, idiotically, cosmically ass backwards. Can you get it that wrong by mistake? Or must you be a willful liar? The lady, after all, was Lieutenant Governor of New York for a moment, which likely puts her in the upper four-fifths of the population in intelligence.
Doctors, she said, will be reimbursed, in part, based on the percentage of their patients who are given end of life counseling. Okay. And, she said, it will also depend on the percentage of cases in which the wishes were carried out. It's at that point that she went off the rails so grandly that, had I not been paralyzed with disbelief, I'd have reached for the remote. And shoved it up my nose. Aiming for my brain.
Her interpretation -- this former politico and self-styled patient advocate -- is that doctors get dinged if their patients change their minds. Really. That's what she said and, apparently, believes. (Okay, she may not believe it: she is, after all, a Republican hack trying to derail health care reform.) You sign an advance directive, that's it. No changes. Any doctor who allows changes gets penalized by THE GOVERNMENT. The lady is an idiot. And, sadly, Jon Stewart didn't call her on it.
Here's the thing: advance directives are for the time when you can no longer make your own decisions. By definition, that means as long as you have the ability, you can change your mind any time you want. In the hospital. In the ICU. Anywhere, anytime. Advance directives are not in effect until you are no longer able to express your wishes. What the bill is doing is making sure doctors follow the patients' expressed wishes when they're no longer able to express them. If a patient has said they want everything done, the doctors must do so. If they've said they don't want to be put on breathing machines, the doctors must honor that request.
It's about following the patients' request. It's about protecting the wishes of patients. I repeat myself. But the lady blew my mind. She couldn't understand her way out of a paper bag.
So this is where we are. This is the level of debate. In a matter as important as this, it's really appalling and disheartening to watch. It's not as if the issues aren't worth discussing. Tying reimbursement to adherence to certain standards is a tricky issue. But if we're going to have the discussion, let's have it with at least a toe still attached to the fundaments. Same with advance directives.
As long as people like that lady get air time without proper rebuttal (in fact, as long as idiocy that deep gets air time at all), we'll never have the kinds of discussions that we need. And deserve.
Tuesday, August 18, 2009
Bureaucrats

Among the many themes of dissent which have gained traction in the health care debate is the canard that we don't wont some government bureaucrat between us and our doctors. Funny thing about that: the only payer entity with which I never had a problem getting authorization for care was Medicare. Here's the sort betweenness I routinely encountered from private insurers:
In the fine print of nearly every private plan are exclusions for "pre-existing conditions." Okay. You had breast cancer, now you can't get any insurance to cover issues related to it. Fair enough, right? Guy's gotta make a buck, right? I mean, it wasn't their fault you got it, right?
But how about this: more than a couple of times I had patients with colon cancer who were denied coverage because of a previous history of.... hemorrhoids!! Yes. Hemorrhoids. Similarly, people who'd had, say, a rubber band placed for hemorrhoids -- a two minute, hundred buck outpatient procedure -- could not get future insurance that would cover ANY disease of the intestinal tract. Band on your butt, screw your stomach. Exit your esophagus. Not, I suppose, that a private insurer has to have any reason for something like that: their goal, after all, is to NOT spend your premiums on your care. Message: if you have hemorrhoids, live with them, baby.
There's more. Many patients of mine whose gallbladders I removed were informed by their insurers that they'd no longer be covered for any disease of their internal organs. A lot of territory excluded, that.
And, as everyone knows, if you lose your insurance because you lost your job, and if you've had any sort of serious illness, you are simply SOL finding new coverage. Imagine the frustration, as a physician trying to help, of dealing with insurance companies as they apply their exclusionary rules. Their rationing. Their death panels.
Yet there they are, those sign wavers, insisting that it's Hitleresque to demand changes in all this. For his attempts, Obama gets branded a Nazi. While the right wing screams, the left wing caves. Advance directives? Gone. Public option? Fuggeddaboutdit. Studies to find out which kinds care work and which don't? Nuh uh. Too... too... I don't know... logical?
I repeat: Medicare, which is in my mind the best paradigm for a public plan, NEVER refused coverage for cancer (or any) care. Not even for grandma. Those government bureaucrats? Not a problem. It was, as anyone might predict, the "market forces" guys who stood between me and my patients.
There is, of course, this little paradox: those people who hate government intervention generally are quite happy with Medicare. Those who point out it's running out of money are those most likely to recoil at suggestions that we ought to find ways of saving money in the program. The ones who think Medicare is shameful socialism would holler "they're trying to raise your taxes!!!" if anyone suggested premiums be scaled to one's financial status.
Is there a more clear example of why we're failing as a country than the debate over health care reform, and the arguments over Medicare in particular?
Thursday, August 13, 2009

Wednesday, August 12, 2009
One Small Step

If anyone here reads Andrew Sullivan's blog, runs across this post, and finds anything familiar in the writing, there could be a reason... Anonymity doesn't do much for blog traffic, but any way to spread the word...
The word, of course, is the extent to which health care reform is aimed at doing things that will be helpful. Even -- especially! -- for those very people who yell and weep and carry guns to meetings, spouting verbatim the insane ravings of Glenn Beck and Sarah Palin while having not the slightest idea what they're really talking about. "Keep government out of Medicare," they say. "Socialism."
The "socialism" trope may be the most laughable (were it actually funny): all of the proposals on the table fall over themselves to maintain the death-grip insurance companies have on us. (Talk about "death panels!" What is it when insurers deny coverage?) None talks about nationalizing the health care delivery system. Not even Medicare is socialism. Single payer -- which in my mind is the only option that makes sense, and which, like Medicare is NOT socialism -- is, clearly, off the table.
There's no possible health care reform package that will satisfy everyone; nor, given the way Congress works, one that will be free of pork-fat, undue complexity, or unexpected consequences that will need to be addressed. Still, what the various iterations seem to have in common are regulations to prevent rescission, to create portability, to remove limits on lifetime coverage, to banish denial for pre-existing conditions. Is it really possible that any of the screamers are against those reforms?
Cost is most certainly an issue, and there is a multitude of ways to address it. Starting, from the doctors' part, with the sort of thing mentioned in that Andrew Sullivan post. Only the surface has been scratched there. And, long after I'm dead, assuming the country still exists, I predict single payer will have come to pass, and people will be glad for it. Even the gun-totin' America lovers.
Signs at the meetings -- ignoring the ones showing Obama as Hitler, a completely ludicrous meme hatched and promoted at Fox "News" (sic) and ingested without chewing by its self-pitying listeners -- point out that Medicare is "bankrupt." While not yet true, it's a point worth considering. To the extent that it hasn't enough money, it's not the fault of Medicare, which spends far less on non-medical expenses than any private insurer. It's because of funding. It's because of the holdover idea from the Reaganomics that you can have what you want without paying taxes.
So, what if everyone were covered by a Medicare-like program, and no one paid premiums; or if there were the sorts of premiums and co-pays associated with Medicare? Currently I pay $14K/year in premiums for me and my wife. Would I be happy to have taxes raised in another area, even, say, by $10K/year? Who wouldn't take that trade? By getting rid of the 30% skim by insurers, that math works right away. And by taking seriously -- instead of demagoging as "death panels" -- the idea of finding cost savings in more efficient care, much more than that will be saved.
And yet, they rave and froth. Getting crazier and scarier. Arguing, in effect, for maintaining a system in which their premiums have likely more than doubled in the last ten years, which covers them sparingly, cutting them off when they need it most: sick, out of work. And they are ready to draw weapons over a plan to pay for help writing the very instructions that will keep them in charge of their care when they're unable to make decisions for themselves.
Who'd have thought people so in need of health care reform could be whipped into a froth by people who lie so freely and make easily refutable claims? I remain unable to understand. And bereft of hope.
Tuesday, August 11, 2009
Local News

Using local anesthesia, I always took care to do it gently, slowly, and thoroughly, and had reason to be proud of the results. Almost routinely, patients expressed their happiness and relief that the process was so... not unpleasant. I've written a bit about it before.
So when I couldn't seem to make someone numb, it hurt. As it were. In addition to having a dissatisfied patient, it made me feel like a failure. It has always been my belief that there are some people who, for some unknown biological reason, process the drugs differently; that it's more than just a few 'fraidy cats or me having a bad day. Now, it seems, there's substantiation. It's those darn redheads.
It never occurred to me to check. I wish I could play back the scenes in my head, in full color. Were the unhappy ones all rubro-capited? There's much I know now that I wish I'd known a few decades ago (and not all of it is surgery-related.) And there've been a few notable redheads in my life. Until now, I've had nothing but happy memories.
Monday, August 10, 2009
Advance Directive

On those few occasions when a patient had an advance directive, it was terrifically helpful. To me as their surgeon, to other caregivers, to the family, and, of course, to the patient. Which is why the outrage over a plan to assist people in making them (and cover the cost of counseling) is as cynical as it is ill-founded. Cynical, because people are turning it into "they're coming to kill grandma." Unfounded, because it actually puts people in control, not caregivers or government.
My parents serve as two examples.
Like most people (or so I assume), my dad had always said he'd never want to be kept alive by machines, and had a directive that put it in writing. Yet when he entered the hospital for what turned out to be the final time, after months of physical decline that had made his life only about the rudiments of existence, when the chips were down he opted for the ventilator. Which is an important point: nothing in his directive prevented him from changing his mind, as long as he could express it. At the time, his world had shrunk entirely, barely extending beyond his skin, having formerly been a man of superior intellect, a voracious reader, adviser to governors and senators, a mayor himself, a judge. Leading up to his death, he'd become unable to get in and out of bed on his own, needed help in all forms of personal care, had not the strength nor will to talk about anything but his own decline. He was miserable. And yet he opted for entry into the critical care unit, where he remained, kept alive, for two futile weeks, until he died. Even having had an advanced directive to the contrary, his wishes at the time were honored, as they should have been. (It did, however, make it easier for everyone, when the futility was evident, to take the steps to discontinue aggressive care. An important point.)
My mom, likely past the midway point in her descent through Alzheimer's disease, also has an advance directive. Composed with the help of her very caring doctor, who gently and carefully went through all the options, it directs that all reasonable measures be taken to prolong her life. Now well past the capacity to consider or reconsider, she gets wonderful care. With her strong heart and good genes, her body will likely live long after her mind is gone entirely.
Whatever else they might mean, these two cases illustrate, at the very least, that making advance directives available is hardly a step down the road to euthanasia.
They also illustrate something else: directives are not for people who retain their ability to make their own decisions. The intent is to carry out people's wishes when they're unable to express them. It's the opposite of euthanasia: it's giving PEOPLE -- not governments or others of evil intent -- legal control over their own fate!! THEIR OWN FATE!!!
The misinformation, willfully disseminated to the vulnerable by those who stand to profit from keeping things as they are, and by those whose only goal is to regain political power no matter the damage to people who need better care, is appalling. But effective. People are scared. They're becoming distrustful of the very thing that allows them to call their own shots beyond the time they otherwise can.
It's the perfect example of how people are being tricked into agitating against the very things they need. That, and the anti-reform protester who was injured at a town meeting, who's now asking for donations. To cover the health care he lost when he lost his job! Simply amazing.
Friday, August 07, 2009
Scam Alert

For months I've been getting spam comments linking to a website called "Findrxonline." I finally took the time to look at it, and find that it requires a monthly subscription which supposedly pays them to find you low-price meds from other websites. As if you couldn't do it yourself.
What a joke. I assume none of my readers is so dumb as to fall for it, but I thought I'd mention it anyway. An outfit that thinks leaving spam on blogs is a good business plan is surely one to avoid. There was another, recently, that responded to my complaint by apologizing. This one not only doesn't do that, but at least one of its email addresses bounces back.
Sigh. For all the beauty of the internet, there must be, it seems, a little ugly too.
Head-Scratcher

I simply don't get it.
Quite aside from the fact that the plan to disrupt health-care town-meetings is overtly to stifle honest debate on a very difficult subject, and despite the fact that there isn't even a bill yet (only a House version and several Senate versions that need reconciling), and even imagining that the anger is real and not ginned up by the distortions and outright lies of the right wing media or fomented by interest groups with a long history of ripping off the health care system for legal profit -- not to mention being fined one point seven billion dollars for fraud -- overlooking all of that: what the hell are these people so mad about?
As far as I can tell, the proposals out there -- the ones that are actually in writing as opposed to the absolutely insane claims of the Rush O'Beckly axis of a$$holery -- are fairly weak-kneed attempts at maintaining the status of most of the quo. Are people really that upset about a bill which aims to prevent their care from being disallowed? Is making insurance portable, and preventing the companies from pulling the plug on coverage when you get sick really that infuriating? In what way is any of it socialism? Do any of the protesters even understand the word?
Yes, there are plenty of problems -- huge problems -- with reforming health care. Which is exactly why the stifling of discussion is so tragic. But can it really be that those screamers and yellers and shouters like things the way they are? Premiums doubling every few years? Losing coverage when they lose a job? Defacto rationing by insurers bent on keeping as much of their money as possible, not spending it on actual health care? Is that what they want? Do they really hate Medicare?
What's so entirely dispiriting is the extent to which these mobs have been whipped up to argue -- once again -- against their own interests. In the most cynical of ways, for the most ignoble of reasons -- ratings, on the one hand, vis a vis the insanity that is Fox News; and pocketbook, on the other hand, vis a vis the insurers who are making billions off the dollars intended to provide medical care -- people have been spun into outrage based on a series of outright lies. Socialism. Coming to kill Grandma. It's unbelievable.
Except that it isn't. Headlong and happily, we're heading off the cliff, cheered on by the very people for whom the system is working fine: making them rich indeed while millions suffer. It shouldn't be possible, it shouldn't be that easy to decieve, but most clearly, it is.
The only thing I can't figure out is this: where do those guys plan to go when this country, at their urging and entirely of their making, is fully down the tubes?
Wednesday, August 05, 2009

{kind=link}
{kind=link}
Tuesday, August 04, 2009
Think Slow

Not too long after setting up shop in this town, I shared a tough case with one of my favorite intensivists. (By way of diversion, I'll add there were only two of them at the time, and they were both my favorites. Practical and canny, surgical-patient-wise, they were a pleasure to work with. Over the years we developed great mutual respect and affection; to the extent that caring for critically ill and deeply challenging patients can be fun, it was.
It's unique to private practice, I think, that such relationships can be so positive and mutually supportive and satisfying. I know I have said that in the academic centers, there's too much turf war and defensiveness. Was, back in the day, anyway. The discovery of such collegiality was one of the pleasures of my entry into private practice.)
To make a long and dimming story short and bright, the patient was an older woman, admitted in extremis to the intensive care unit. Dying, evidently, of infection of indeterminate source. Clearly, she had severe pneumonia. Was there anything else? I was consulted early on, charged with ruling in or out a surgical and operable cause of her illness.
Without going into details (mostly because I can't remember them), I became convinced that the lady's decline was not due to any kind of "surgical" condition. I continued to follow her three or four times daily, during which time the intensivist in charge kept working me over: she's dying; at least have a look inside to see if there's anything fixable. For those unremembered reasons, I continued to resist. At some point it became moot. If I'd been wrong and she indeed had a surgically treatable condition, she'd ultimately descended beyond her ability to recover from whatever I might do.
Young, and not much established in the community, I didn't find it at all easy. The phrase lobbed to me more than a few times was, "It's time to fish or cut bait." I was well aware that if I was wrong it could be awful: for the patient, of course, but very likely for me, too.
Not a good enough reason. It's not unreasonable sometimes, when all else fails, to "have a look." Before the ready availability of quite accurate non-operative testing, such an undertaking (as it were) was not entirely rare. In this case, certain as I was, I simply didn't want to do it. Not absent from my thinking was the realization that if I did operate against my better judgment, and found nothing to fix, I would have become, in a very real sense, her executioner.
If anyone has the answer to such dilemmas -- which, I might say, we still face despite our imaging capabilities -- I'd be happy to hear it. Meanwhile, in the case at hand, the unfortunate lady died.
With more than a little dread, I awaited the autopsy findings, and came to have a look when it happened. (There's another subject: autopsies are done increasingly rarely nowadays. This case is an excellent example of why they are still needed.) I'm happy (if that's the right word) to report that it confirmed my conclusion that she did not have any pathological process going on in her belly.
There's really no lesson to the story, other than sort of confirming my belief that more mistakes are made in operating too hastily than in giving things time to sort out -- assuming there IS time. But the real point is that for the next twenty years of an extraordinarily productive and rewarding relationship between myself and the intensivist, the phrase fish or cut bait was used uncountable times. With varying meanings, depending on who said it, where, and why.
It's unique to private practice, I think, that such relationships can be so positive and mutually supportive and satisfying. I know I have said that in the academic centers, there's too much turf war and defensiveness. Was, back in the day, anyway. The discovery of such collegiality was one of the pleasures of my entry into private practice.)
To make a long and dimming story short and bright, the patient was an older woman, admitted in extremis to the intensive care unit. Dying, evidently, of infection of indeterminate source. Clearly, she had severe pneumonia. Was there anything else? I was consulted early on, charged with ruling in or out a surgical and operable cause of her illness.
Without going into details (mostly because I can't remember them), I became convinced that the lady's decline was not due to any kind of "surgical" condition. I continued to follow her three or four times daily, during which time the intensivist in charge kept working me over: she's dying; at least have a look inside to see if there's anything fixable. For those unremembered reasons, I continued to resist. At some point it became moot. If I'd been wrong and she indeed had a surgically treatable condition, she'd ultimately descended beyond her ability to recover from whatever I might do.
Young, and not much established in the community, I didn't find it at all easy. The phrase lobbed to me more than a few times was, "It's time to fish or cut bait." I was well aware that if I was wrong it could be awful: for the patient, of course, but very likely for me, too.
Not a good enough reason. It's not unreasonable sometimes, when all else fails, to "have a look." Before the ready availability of quite accurate non-operative testing, such an undertaking (as it were) was not entirely rare. In this case, certain as I was, I simply didn't want to do it. Not absent from my thinking was the realization that if I did operate against my better judgment, and found nothing to fix, I would have become, in a very real sense, her executioner.
If anyone has the answer to such dilemmas -- which, I might say, we still face despite our imaging capabilities -- I'd be happy to hear it. Meanwhile, in the case at hand, the unfortunate lady died.
With more than a little dread, I awaited the autopsy findings, and came to have a look when it happened. (There's another subject: autopsies are done increasingly rarely nowadays. This case is an excellent example of why they are still needed.) I'm happy (if that's the right word) to report that it confirmed my conclusion that she did not have any pathological process going on in her belly.
There's really no lesson to the story, other than sort of confirming my belief that more mistakes are made in operating too hastily than in giving things time to sort out -- assuming there IS time. But the real point is that for the next twenty years of an extraordinarily productive and rewarding relationship between myself and the intensivist, the phrase fish or cut bait was used uncountable times. With varying meanings, depending on who said it, where, and why.
Subscribe to:
Posts (Atom)
Sampler
Moving this post to the head of the list, I present a recently expanded sampling of what this blog has been about. Occasional rant aside, i...

-
 Moving this post to the head of the list, I present a recently expanded sampling of what this blog has been about. Occasional rant aside, i...
Moving this post to the head of the list, I present a recently expanded sampling of what this blog has been about. Occasional rant aside, i... -
 I finished the previous post with the sad story of my patient, illustrating diagnostic difficulties at the fringes of biliary disease. An...
I finished the previous post with the sad story of my patient, illustrating diagnostic difficulties at the fringes of biliary disease. An... -
 Warning: here follows a rant that some will find offensive, but which is medically-related, so I'm doing it. Turn back now, if you have ...
Warning: here follows a rant that some will find offensive, but which is medically-related, so I'm doing it. Turn back now, if you have ...