
Among the many themes of dissent which have gained traction in the health care debate is the canard that we don't wont some government bureaucrat between us and our doctors. Funny thing about that: the only payer entity with which I never had a problem getting authorization for care was Medicare. Here's the sort betweenness I routinely encountered from private insurers:
In the fine print of nearly every private plan are exclusions for "pre-existing conditions." Okay. You had breast cancer, now you can't get any insurance to cover issues related to it. Fair enough, right? Guy's gotta make a buck, right? I mean, it wasn't their fault you got it, right?
But how about this: more than a couple of times I had patients with colon cancer who were denied coverage because of a previous history of.... hemorrhoids!! Yes. Hemorrhoids. Similarly, people who'd had, say, a rubber band placed for hemorrhoids -- a two minute, hundred buck outpatient procedure -- could not get future insurance that would cover ANY disease of the intestinal tract. Band on your butt, screw your stomach. Exit your esophagus. Not, I suppose, that a private insurer has to have any reason for something like that: their goal, after all, is to NOT spend your premiums on your care. Message: if you have hemorrhoids, live with them, baby.
There's more. Many patients of mine whose gallbladders I removed were informed by their insurers that they'd no longer be covered for any disease of their internal organs. A lot of territory excluded, that.
And, as everyone knows, if you lose your insurance because you lost your job, and if you've had any sort of serious illness, you are simply SOL finding new coverage. Imagine the frustration, as a physician trying to help, of dealing with insurance companies as they apply their exclusionary rules. Their rationing. Their death panels.
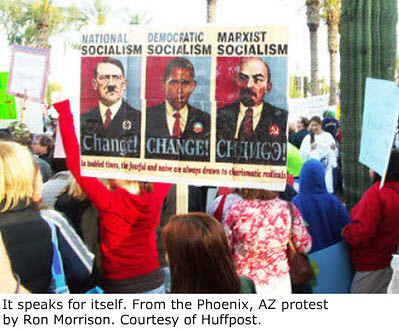
Yet there they are, those sign wavers, insisting that it's Hitleresque to demand changes in all this. For his attempts, Obama gets branded a Nazi. While the right wing screams, the left wing caves. Advance directives? Gone. Public option? Fuggeddaboutdit. Studies to find out which kinds care work and which don't? Nuh uh. Too... too... I don't know... logical?
I repeat: Medicare, which is in my mind the best paradigm for a public plan, NEVER refused coverage for cancer (or any) care. Not even for grandma. Those government bureaucrats? Not a problem. It was, as anyone might predict, the "market forces" guys who stood between me and my patients.
There is, of course, this little paradox: those people who hate government intervention generally are quite happy with Medicare. Those who point out it's running out of money are those most likely to recoil at suggestions that we ought to find ways of saving money in the program. The ones who think Medicare is shameful socialism would holler "they're trying to raise your taxes!!!" if anyone suggested premiums be scaled to one's financial status.
Is there a more clear example of why we're failing as a country than the debate over health care reform, and the arguments over Medicare in particular?




{kind=link}
{kind=link}
29 comments:
Hi! This is a reply to both this post and the one about the $15000 needle. I'm a newly graduated doctor in Sweden. It's traditionally a democratic socialist country (at least in theory), although at the moment the conservatives rule (don't be fooled, they're more to the left than your democrats). That sign you link to strikes me as funny, because if I were to, very briefly, compare our system to yours, they're quite similar. Everyone pays up to $125 for medical care, and up to $250 for prescription drugs every year, after that it's all free (though everyone also earns less, so the above figures could be slightly misleading). Of course the bill goes somewhere, and so it's up to the provider to try and keep the cost down. It works, although with the recent tax cuts and people getting older etc, it's getting a bit stretched. We'll see where it's headed. I just thought that sign was "interesting". And the current debate in the US too. Although a little frightening. Keep posting, I really enjoy reading this blog (and the other one, too)! Warm regards from Socialist Sweden.
As I posted on my blog, my 23-year-old just got refused private insurance, now that she's aged out of ours. One of their stated reasons was because she had a cataract at age 7, and another was, because--get this--she had cataract surgery at age 7. Wait--huh?!
I think the real reason is, we're paying COBRA on her and that same company is getting nearly four times the premium for the same coverage on the same person. So why would they want to give that up? And why would they care if she gets thrown out in 15 months when COBRA ends?
Johannes: thanks for your comment. Wish I could read the recipes on your blog. They look delicious!
Wow, Medicare must truly be wonderful. No mention at all of their terrible payment rates or BS documentation requirements that have singlehandedly destroyed charting in our health care system (soon after, like all terrible Medicare ideas, adopted by private insurance). Or of their growing habit of auditing practices and hitting people with 50k+ government fines for ts they deem improperly crossed. Can't wait till they're the only game in town, they certainly show no signs of abusing that power.
From the patients' point of view, it IS pretty wonderful. And, since it is a government program, it is ultimately responsive to input from voters, which is not true of private insurers, working with whom is no less onerous for physicians.
There is no system, real or imagined, that will be perfect all the time for all people. The question is, does the current system work and is it sustainable without significant change? In my view, the answer is clearly no. So, then, how would you change it? How would you address costs that are rising at rates that will bankrupt us?
My fear is that, if the health care budget for the US is one number on one line in the budget, it is, as George Will would probably say, open to mischief. It could be a balancing account for the rest of the budget. It might be too low, leading to a "don't get sick after May" mindset. It will never be too high. What should the number be, do you think?
--A Better Angel
A fair question, ABA, and one which ought to be addressed openly. How much can we afford to/do we wish to spend as a nation on health care? What would that cover? Would knowing #2 alter the answer to #1?
Should it be in terms of actual dollars, or expressed as a percent of budget?
Here's an excellent article, which is pretty long and comprehensive and, at the end, presents an interesting solution.
It's also true that rest of the budget ought to be addressed in the same way; particularly military spending. Indexing social security and medicare ought to be on the table, too.
Those darn sign wavers!
http://www.zombietime.com/zomblog/?p=621
pilpusherl
pilp, I couldn't get your link to work. But I'm sure it illuminated the issue of insurance companies denying coverage, and of the way in which people have been tricked into protesting, against their own interests, attempts to fix it.
great point of view. regarding medicare - i likewise have never had to interrupt my already excruciatingly busy day for a "peer-to-peer" review of my medical decision making as another private medical director denies an MRI.
mind if i include this in grand rounds this week?
I'd be honored, Dr Charles.
I'd be curious to read your reaction to the surgeon who wrote in the Washington Post: http://www.washingtonpost.com/wp-dyn/content/article/2009/08/19/AR2009081903189.html?nav=hcmoduletmv
Alison: there's nothing really new in the article. I agree with much of it: there are indeed problems with the sorts of "scoring" that is done on practice parameters, for example. On the other hand, there are some examples that, as far as I know, are not based on any actual plans under consideration.
I've written about the negative impact of declining reimbursements and lack of recognition for those that do a better job than others. On the other hand, he spends a lot of time on the misstatements Obama made which, although annoying, don't really reflect what he meant. The tonsil thing, eg.
I think there is a lot of bad behavior by some doctors, and costs generated either willfully or inadvertently, by way of not knowing better. It's an area that needs addressing. If there weren't huge differences between the practices of doctors, rules wouldn't be necessary. But there are, and they are. The problem -- and I agree with the implication of the article -- is that when rules are made and implemented, there are always adverse consequences; especially in something as far from black and white as the practice of medicine.
Thanks for sharing your thoughts about the current (and insane) health-care reform debate from your uniquely qualified perspective. If only the media treated this crisis with the seriousness it deserves instead of covering the ongoing circus freak show that the private insurers (and their allies) have directed the discourse into.
That the media chooses to amplify voices of angry TEA participants and conservative pundits (parroting out-of-date talking points) at the exclusion of the voices of patients and doctors tells me this country is in for a bumpy ride. The media's complicity in this nonsense is like the hamstringing of the Clinton Presidency all over again, or like the big sell of the Iraq War. I fear for this country.
anonymous: me, too. This will be the year, I think, that historians (if there are any left) will point to as the one that showed finally, inarguably, that our politics became too dysfunctional ever to work again.
I understand your eagerness to hate insurers, but you're ignoring the drivers of healthcare costs: provider's incomes, high tech treatment, high cost procedures, high drug costs, etc. Insurance is a reflection of these costs, not a driver.
If you believe expansion of Medicare is the solution that leads us to the nirvana experienced by social systems, that's a fantasy - unless you're ready to make the right changes. Right now we spend (as a % of GDP) almost the same as the average OECD country does on publicly financed healthcare (Medicare, Medicaid,etc.). The difference is we're only covering the old and the poor while the social systems are (supposedly) covering ALL of their people.
Medicare is going broke despite the cost shifting providers do to those with private insurance. And that's supposed to be the basis for reducing costs? What a joke.
If you want to go the social system route, first make all the providers employees of the government and mandate their wages to be no more than their counterparts in the other social systems. Then reduce heart surgeries, cat scans, pharma spending, etc. to the same levels as socialized systems. Be sure to eliminate the hospital practices of unbundling charges and having $75,000 markups on a $10,000 pacemaker they have delivered the day of the surgery. Then eliminate physician ownership of clinics providing support services so there's no incentive to receive compensation by ordering additional treatment. Also, be sure to anticipate the same waiting lists pervasive in the socialized systems.
Sounds great, right? I'm sure you'd agree to those changes for the sake of a better system that eliminates insurers.
Brian: it's not about "eagerness" to hate insurers, it's about reasons to do so. Medicare is going broke, in large part, because if the way it's funded, not because it (unlike insurers) is sucking 30% of the health care dollars out of the system. You make clever snarky arguments. How about a decent suggestion? How about telling us what, exactly, insurance companies add to the health care system that is worth keeping?
After years of decrying the excess costs of Medicare, when a president actually says he'll do something about it, Republicans suddenly cry he's trying to destroy it and they're the ones who'll save it. Now THAT'S a joke!
There are lots of ways to address costs of health care in this country. How nice it would be if the "opposition" would join in, instead of making up "death panels" and "government telling your doctor what she can do" sorts of drivel.
You use heart surgery as an example, suggesting that other countries offer it too infrequently, if I understand your non-snark from your snark. Might it be the opposite? Might there, indeed, be merit in the idea of looking more closely at what appropriate indications are, when other interventions are more effective?
These are the sorts of things Obama has suggested and which are being reflexively shouted down by the likes of Glenn Beck, who wouldn't know a fact if it pulled down its pants and sat on his face.
Show us the evidence that "competition" among insurers has held down costs. Show us the benefit of having them standing between patients and providers, as opposed to a single payer. Respond to my point, which was that private insurers try all the time to refuse to pay for legitimate and needed care, and medicare doesn't.
Focus your outrage. Settle down and add something to the discussion.
Sid, it's not snarkiness to listen to ridiculous points that address nothing and instead simply try to find a bad guy to get an agenda through and avoid having the spotlight on themselves. You call my points "clever snarky arguments". That sounds very close to 'arguments I can't refute but will try to deflect'.
Even though you totally ignored the points I've already given, let's go through this:
Medicare: The myth of Medicare's effective administration is that it does everything for a mere 3% overhead. This is an example of a fact that doesn't represent the truth. I could go through all of this but here's a link that details the truth: http://www.heritage.org/research/healthcare/wm2505.cfm
The bottom line is this: In 2005, Medicare's admin costs were $509 per primary beneficiary, compared to $453 for insurance companies - and that includes insurance company profits.
So, one answer about what insurance companies provide is better, far more cost effective administration than the government.
Another is it avoids the rampant fraud in Medicare. As you pointed out, Medicare never refuses payments. Do you honestly believe those are all legitimate charges? I understand providers don't like someone reviewing their bills but too bad.
Private insurance also helps by avoiding the special interests that want enhanced (mandated) coverage for their particular practice or 'benefit'. Reference the argument over whether the NHS should pay for Viagra, or how you have each state (and under Obama the feds) dicating where the money should be spent. That's just so corrupt to have providers, drug companies, etc. hiring a lobbyist to get the government to mandate their particular service is paid. That's what we're heading to with government care.
Suggestions for reform: You claim there are lots of ideas for cost control and I should give a few - while directly ignoring all of those I gave. Why is that? I believe because my suggestions directly address the cost drivers of healthcare - providers, drug companies, etc. I think that's why you pointedly ignored them.
Here are some more you can ignore:
First, we don't have competition amongst insurers (in most cases). However, the reasons for that are not because the vast majority of insurers don't want to compete. Right now the regulators create 51 barriers to entry that keep most insurers out of most states.
Second, the regulators mandate coverage based upon the special interests of the providers that run up the cost.
Third, providers - most likely like you - give discounts to the large insurers that make it impossible to compete. Here's the scenario: Same surgery, two insurers - one big and one small. Do you issue the same bill? Probably. Do you give the same discount? If you do you're the only one in the country that does.
This is like asking a store to compete with Walmart but telling them their cost of goods is always going to be 35% higher than Walmart's. You providers have created the lack of competition by giving lower cost of goods to Blue Cross, United, Cigna, and Aetna than any small company can get.
If you want competition just do the following:
1. Allow cross state border purchase of insurance without state mandated benefits.
2. Prohibit providers from offering more than a 5% discount difference to any party over another. Better yet, just mandate the pricing at no more than 10% over the Medicare reimbursement rates.
Continued in next post.
Continued
A couple of other points:
You try to lump me in with those opposed to ObamaCare by claiming I'm somehow arguing about death panels. Please point out where I did that, or I'll assume that's another deflection.
You also missed my point about heart surgeries. It's not that other countries offer them too little, but that we offer them too much. We now have huge hospitals dedicated to providing surgeries. Should we really believe we're getting the right diagnosis from the surgeon when the only way they make money is by doing surgery? And, the overhead of the hospital doesn't exactly get paid by finding or giving an alternative treatment that doesn't involve cutting someone, does it? I'm sorry about being snarky again by pointing out those inconvenient truths.
You've unintentionally given your own illustration of how insurers hold down costs compared to a single payer. Here it is:
As you state, insurers deny coverage for things you want covered. Those things include experiemental treatments that haven't been proven effective, duplicate charges, unbundled charges, treatment that's not medically necessary, etc. It is ironic that you applaud Obama reviewing care effectiveness but deplore this when it's done by insurers. (I understand that's only a portion of what you hate about insurers, but I'll address that shortly.) Not to be snarky, but care to address the apparent hypocrisy?
It should also be noted that insurers NEVER deny any treatment. Only providers refuse to actually provide it. You're just lamenting that, unlike Medicare, insurers put restrictions on what it will pay - while applauding the idea that Obama would have the government do the same thing.
This also results in the demonstration of why insurers are far more cost effective than the single payer when done it's done right. Under the single payer system that we have - Medicare and Medicaid - we cover a third of the population and spend 45% of our healthcare money. This doesn't even take into account that Medicare gets the best pricing possible and providers shift huge costs to private insurers. It's really outrageous to even hint that single payer is more effective in the US.
Why not try to make the single payer we have effective and not bankrupt before expanding it? (Snarkiness alert) I guess it's too much to ask the government to actually prove it can do what it says before expanding a bankrupt program.
Finally, I wholeheartedly agree there should be health insurance reform. The difference is (and this is not snarkiness) I believe it should be done effectively. How is that done? It's simple. Mandate insurance coverage, eliminate most mandated benefits, issue a minimum coverage standard, provide premium support for those that can't afford the base premiums, require insurers to provide initial coverage and conversion plans for new enrollees, allow cross border purchage, allow any level of coverage as long as the minimum is offered, etc.
I believe I've responded to every point you made. If not, point it out and I'll respond. I'll also expand on the insurance reform tomorrow but what I've proposed would quickly eliminate at least 90% of your objections and the problems with insurance.
Wow, Brian, that's a lot of wrong to address. But since you are making an effort, even if entirely off base, so will I.
Sid, it's not snarkiness to listen to ridiculous points that address nothing and instead simply try to find a bad guy to get an agenda through and avoid having the spotlight on themselves.
Once again you imply I'm looking for a bad guy. I'm pointing out issues.
You call my points "clever snarky arguments". That sounds very close to 'arguments I can't refute but will try to deflect'.
Well, what would you call your penultimate paragraph? Were you seriously suggesting socializing the health care delivery system? If so, you're about the only one on either side of the argument.
Even though you totally ignored the points I've already given, let's go through this:
Medicare: The myth of Medicare's effective administration is that it does everything for a mere 3% overhead. This is an example of a fact that doesn't represent the truth. I could go through all of this but here's a link that details the truth: http://www.heritage.org/research/healthcare/wm2505.cfm
the heritage foundation is hardly a non-partisan outfit, nor free of corporate influence. For every study like that, there are tens of these.
The bottom line is this: In 2005, Medicare's admin costs were $509 per primary beneficiary, compared to $453 for insurance companies - and that includes insurance company profits.
Not credible unless you show the math
So, one answer about what insurance companies provide is better, far more cost effective administration than the government.
Simply untrue. With 1200 companies, each with CEOs many of whom make tens of millions, shareholders getting dividends, money spent on advertising, lobbying -- not to mention the tens of thousands of employees trying to keep from spending your money, and the tens of thousands of hospital and physician employees trying to make them pay, the costs are enormous compared to Medicare.
Another is it avoids the rampant fraud in Medicare. As you pointed out, Medicare never refuses payments. Do you honestly believe those are all legitimate charges? I understand providers don't like someone reviewing their bills but too bad.
I said no such thing. I said "legitimate and needed care."
Private insurance also helps by avoiding the special interests that want enhanced (mandated) coverage for their particular practice or 'benefit'. Reference the argument over whether the NHS should pay for Viagra, or how you have each state (and under Obama the feds) dicating where the money should be spent. That's just so corrupt to have providers, drug companies, etc. hiring a lobbyist to get the government to mandate their particular service is paid. That's what we're heading to with government care.
So it's your position that insurance companies are better in that they cover less? And you're ignoring the lobbying going on right now by drug companies to defeat allowing the government to issue competitive bid? And the money insurers are spending to defeat legislation compelling them to cover pre-existing conditions or to stop kicking people out when they get sick? That's not corruption in your view?
Suggestions for reform: You claim there are lots of ideas for cost control and I should give a few - while directly ignoring all of those I gave. Why is that? I believe because my suggestions directly address the cost drivers of healthcare - providers, drug companies, etc. I think that's why you pointedly ignored them.
No, I ignored them because I took them to be unserious. But if you really are in favor of government controlling how hospitals bill and preventing docs from owning clinics, then you're beyond liberal. You're a socialist. But then, you seem not to like the NHS. I can't figure it out.
Here are some more you can ignore:
First, we don't have competition amongst insurers (in most cases). However, the reasons for that are not because the vast majority of insurers don't want to compete. Right now the regulators create 51 barriers to entry that keep most insurers out of most states.
In my state there are dozens of insurers. That's competition. My point is that it hasn't caused lower costs or better benefits for subscribers. Collusion, maybe? They sure as hell don't want the kind of real competition that a public option would represent.
Second, the regulators mandate coverage based upon the special interests of the providers that run up the cost.
No idea what you mean there..
Third, providers - most likely like you - give discounts to the large insurers that make it impossible to compete. Here's the scenario: Same surgery, two insurers - one big and one small. Do you issue the same bill? Probably. Do you give the same discount? If you do you're the only one in the country that does.
This shows how little you know. It's actually breathtaking in its wrongness. By law, if I were to submit different bills to different payers for the same service, I'd have committed a felony, a crime against Medicare. Punishable by fines and prison. I can't even offer a discount to an uninsured patient. Moreover, insurers have steadily cut what they pay providers, and made it a condition of acceptance that the difference between the "bill" and what's reimbursed cannot be collected. You couldn't be more wrong about any of this.
This is like asking a store to compete with Walmart but telling them their cost of goods is always going to be 35% higher than Walmart's. You providers have created the lack of competition by giving lower cost of goods to Blue Cross, United, Cigna, and Aetna than any small company can get.
Complete and utter bullshit, totally backwards.
I
If you want competition just do the following:
1. Allow cross state border purchase of insurance without state mandated benefits.
Fine with me. Who's against it, and why?
2. Prohibit providers from offering more than a 5% discount difference to any party over another. Better yet, just mandate the pricing at no more than 10% over the Medicare reimbursement rates.
See above. Total complete astonishing misunderstanding of reality.
You try to lump me in with those opposed to ObamaCare by claiming I'm somehow arguing about death panels. Please point out where I did that, or I'll assume that's another deflection.
Please point out where I did that. I referred to "the opposition," which, in context, refers to the politicians standing in the way of reform.
You also missed my point about heart surgeries. It's not that other countries offer them too little, but that we offer them too much. We now have huge hospitals dedicated to providing surgeries. Should we really believe we're getting the right diagnosis from the surgeon when the only way they make money is by doing surgery? And, the overhead of the hospital doesn't exactly get paid by finding or giving an alternative treatment that doesn't involve cutting someone, does it? I'm sorry about being snarky again by pointing out those inconvenient truths.
Huh? Isn't that exactly what I said: looking into why we do more, finding out what alternatives might be better? As Obama suggests, and as the right wing characterizes as rationing or death panels.
You've unintentionally given your own illustration of how insurers hold down costs compared to a single payer. Here it is:
As you state, insurers deny coverage for things you want covered. Those things include experiemental treatments that haven't been proven effective, duplicate charges, unbundled charges, treatment that's not medically necessary, etc. It is ironic that you applaud Obama reviewing care effectiveness but deplore this when it's done by insurers. (I understand that's only a portion of what you hate about insurers, but I'll address that shortly.) Not to be snarky, but care to address the apparent hypocrisy?
What hypocrisy? Nowhere did I argue against denying duplicate charges, fraud, etc. I described denying needed coverage for colon cancer because a patient had had prior hemorrhoids. The two are as different as they could be, and there's no hypocrisy at all.
It should also be noted that insurers NEVER deny any treatment. Only providers refuse to actually provide it. You're just lamenting that, unlike Medicare, insurers put restrictions on what it will pay - while applauding the idea that Obama would have the government do the same thing.
If you believe insurers NEVER deny treatment, you are simply refractory to all the evidence out there, and are, I guess, calling me a liar. In which case, I'm wasting my time giving you thoughtful answers.
This also results in the demonstration of why insurers are far more cost effective than the single payer when done it's done right. Under the single payer system that we have - Medicare and Medicaid - we cover a third of the population and spend 45% of our healthcare money. This doesn't even take into account that Medicare gets the best pricing possible and providers shift huge costs to private insurers. It's really outrageous to even hint that single payer is more effective in the US.
You've made one of the best arguments for single payer for all. Same prices, no cost shifting.
Why not try to make the single payer we have effective and not bankrupt before expanding it? (Snarkiness alert) I guess it's too much to ask the government to actually prove it can do what it says before expanding a bankrupt program.
Finally, I wholeheartedly agree there should be health insurance reform. The difference is (and this is not snarkiness) I believe it should be done effectively. How is that done? It's simple. Mandate insurance coverage, eliminate most mandated benefits, issue a minimum coverage standard, provide premium support for those that can't afford the base premiums, require insurers to provide initial coverage and conversion plans for new enrollees, allow cross border purchage, allow any level of coverage as long as the minimum is offered, etc.
Pretty much the Baucus plan. It's probably the best we can get. It's also a gift to insurance companies to the tune of billions of dollars that could have gone directly to health care.
I believe I've responded to every point you made. If not, point it out and I'll respond. I'll also expand on the insurance reform tomorrow but what I've proposed would quickly eliminate at least 90% of your objections and the problems with insurance.
Please don't. You have shown such a poor understanding of how things are that I don't want to waste more time trying to correct you. Your statements indicate you won't be impacted by anything I say.
Sorry Sid, I don't mean to offend you by pointing out truths that counter your beliefs.
I also apologize for doing two separate posts again.
A few quick points: State regulators, those that want socialized medicine, and large insurers who are able to keep control of the market are those opposed to allowing the sale of insurance across state borders.
I'm not advocating socialized medicine but pointing out the only way single payor addresses the cost of healthcare is if you make providers employees of the government, hospitals government owned, etc. Otherwise you're not addressing the cost drivers and only blaming the party reflecting those costs.
Even if we accept your posted admin study as factual (which I don't) it still leaves a hard gap to explain. It says Canada spends 16.7% on admin compared to 31% by insurers. My rough math shows that if we reduce our admin level to that amount we're still spending 50% more than Canada does per capita. Hmmm. Where does all the other money go and why aren't we addressing that in this debate that switched from healthcare reform to health insurance reform?
I'll say this again: Insurers can't deny treatment because they don't provide treatment. Providers can still give treatment if the insurance company won't pay for it. Insurers certainly deny PAYMENT for certain treatments or for initial coverage - and I have no problem addressing those issues. But what you seem to want is insurers to pay providers for treatment that isn't eligible under the contract.
BTW, many times this is what happens: People who are uninsured who suspect they have a condition apply for insurance and don't disclose the conditions. They claim for coverage and the insurer finds out it is a pre-existing condition. For those that have been responsible insurers should have the responsibility for continuing coverage - as I pointed out in my previous post. For those that haven't been responsible, the insurer owes it to those that have maintained coverage not to increase their premiums by paying claims on conditions that were not disclosed.
Bad faith claims against health insurers is a lawyers fantasy so insurers are pretty sure of the facts before they deny coverage. Once again, I don't mind constructive changes but laments about how insurers live by contracts when everyone else has to is a deflection.
It is interesting that you call me a socialist because I suggest billing levels being controlled by the government. Uh, what do you think Medicare does - and that seems to be what you want to expand. I'm simply suggesting that you expand that level of reimbursement to everyone - and I'm surprised to see you don't want that competition.
Which leads to what I can't let go without a challenge because it's the biggest single hindrance to competition:
My quote:
Third, providers - most likely like you - give discounts to the large insurers that make it impossible to compete. Here's the scenario: Same surgery, two insurers - one big and one small. Do you issue the same bill? Probably. Do you give the same discount? If you do you're the only one in the country that does.
Your response:
"This shows how little you know. It's actually breathtaking in its wrongness. By law, if I were to submit different bills to different payers for the same service, I'd have committed a felony, a crime against Medicare. Punishable by fines and prison. I can't even offer a discount to an uninsured patient. Moreover, insurers have steadily cut what they pay providers, and made it a condition of acceptance that the difference between the "bill" and what's reimbursed cannot be collected. You couldn't be more wrong about any of this."
Sid, you make no sense here because you claim I'm completely off base and then agree that providers are reimbursed different levels. It appears you're trying to deflect what is done in every single hospital and providers office across the country. If you're seriously trying to say providers receive the same amount of money from everyone for the same service, well, in this case I have to call you a liar.
Notice I specifically said in my quote that you'd have the same bill, but different levels of reimbursement. You then claim I'm trying to say you submit different bills for the same treatment. How snarky.
Typically, this is how it works: A provider bills for treatment. There is a level of reimbursement offered by Medicare that is normally the lowest. There are contracts providers hold with the largest insurers that are the lowest private reimbursement levels. Providers then have contracts with other PPO's (First Health, Beechstreet, etc.) that are given discounts but not to the level of the larger insurers. To deny that is, as you say, utter bullshit.
Here's the direct question: If a hospital submits a bill for the same amount for the same service to Medicare, a large insurer that it holds a contract with, and a small insurer that it doesn't have a contract with, are you claiming the hospital will always be reimbursed the same amount by all three payers?
Brian, your ability to twist is as impressive as an Olympic gymnast.
Your quote:
Sid, you make no sense here because you claim I'm completely off base and then agree that providers are reimbursed different levels. It appears you're trying to deflect what is done in every single hospital and providers office across the country. If you're seriously trying to say providers receive the same amount of money from everyone for the same service, well, in this case I have to call you a liar.
Of course providers are reimbursed at different levels; but you said it was because they "give" discounts to insurers. It's simply not the case. Insurers say to providers, "this is what we pay. Take it or leave it." Not wanting to lose patients, providers take it. There's no "giving" of a deal by providers. It's taking the latest screw job. Which answers your final question as well.
This gets to another crucial matter: so far, cost control has only been in the form of cutting payments to providers. Obama has suggested looking where there real money is, by finding what works and what doesn't, how some docs are able to get better results at lower costs than others. THAT'S what I've argued for for years.
Nor do I disagree that in some ways single payer would be bad for docs, unless it's set up right (as I've written on this blog). But, without any doubt at all, it will be better for patients, and that's the bottom line. Done right, there'd be no need to cut payments further to providers; in fact, the better ones could see their incomes go up.
For Brian.
Thanks for dropping by, Brian. I'm tired of your inability to accept the actual meaning of words. Have a nice day.
Post a Comment