
Above all, interns love the fast surgeons. The longer an operation takes, the less time to do your work when finally released from the tiled temple. A whole OR day with a plodder guarantees a night without sleep. There are other reasons to appreciate fast surgery, and to consider why some surgeons are so much faster than others. But before doing so, let this be made clear: speed, per se, is not a sine qua non (or even the sine qua not much) of good surgery. Doing it right is paramount; a slow and careful surgeon is better than a fast and sloppy one.
An operation done fast, when done well, is better than a proper but slow one. Not often, necessarily: but given the ill effects of anesthesia, the additive impact of tissue trauma, fluid shifts, exposure of uncovered tissues to the elements, all other things being equal, the less time in the OR the better. Over a lifetime of procedures, I think it fair to say fast surgeons will have fewer complications than slow ones. Especially with critically ill or elderly patients.
Although I like much better the other images it conjures, "skin to skin" refers to the actual time of an operation -- from cutting the skin to finishing sewing it up. (Total OR time is longer -- often much longer -- depending on OAFAT and other issues.) Usually only invoked when it's good news, it's like this: "How'd the Whipple go?" "Two hours, skin to skin!" When not so good, it's "Oh man, it took forever..." Skin to skin -- as it should -- connotes goodness.
Vic Richards was the fastest surgeon I'd known. (Lots more about him in my book.) Former chief of surgery at the Stanford program when it was still in San Francisco, he'd gotten his MD at age 19 (!) and was chairman at age 30. Right after getting his degree, too young to do much else, he worked in an anatomy research lab, where he ended up teaching surgery residents much older than he. In the process, he figured out subtleties of anatomy previously not well-known, and thought about how to do things in the operating room based on his anatomic insights.
By the time I knew him he was well-established as one of San Franciso's premier surgeons, loosely associated with UCSF, where I was training. I spent some months with him as chief resident, and he opened my eyes -- although I think it wasn't until I'd been in practice at least a couple of years that I really understood what he'd shown me. "Slow down, Dockie," he'd say. "You're going too fast. I'm the slowest surgeon in town...." In one sense, he was: his hands were not a blur; he didn't tie knots so fast you couldn't see the moves, didn't flash his knife like a Ninja. His speed -- usually he took half the time of the professors who'd theretofore taught me -- came from his head, not his hands.
I can't quantify it. Fast surgery is greater than the sum of many important parts. Every move ought to make sense, and flow logically from the previous one. For that to be true, you need a global idea of what it is you need to do, and the idea has to be a good one. That's for starters. Clearly, you need certain basic skills; you need to understand the relevant anatomy; but also you need -- here it gets a little nebulous -- an instinct for economy of movement and for what makes sense. To clarify what I mean (if not necessarily to shed more light): I've assisted many surgeons on complex operations wherein we came to a point at which I felt I knew what the next move ought to be, only to see the surgeon go somewhere else. "Look at that!; isn't that something?; he had it and he lost it! He's not seeing it!"
That's what Vic would have said, in his non-stop running commentary on everything I was doing under his tutelage. Assisting, in those early practice days, I'd say nothing and do what I could to help with the new path. Eventually, the paths converge. It's not as if there is one and only one sequence of events for a given operation. The surgeons who take four steps where one might suffice are not bad surgeons, generally. We all benefit from the incredible resilience of the human body. If we get things pretty close, it'll do the rest.
But little things add up. Some surgeons are so wedded to specific instruments, for example, that if it's not available they'll stop everything in the middle of an operation while someone gets it. It's almost always the case that something else would do. It's desirable to have a predictable routine for any operation; it's not desirable to be unable to deviate from it. On the other hand, some routines themselves are counterproductive. You can make a midline abdominal incision, as an example, and be into the peritoneal cavity literally in a minute or less; or you can do it in a way that takes ten, using cautery, slow-cooking your way through the fat, leaving non-viable (yeah, but non-bleeding, they'll tell you) tissue in your wake. Any operation provides many such opportunities.
Maybe most important of all, and least understood, is knowing when you are in exactly the right plane, as opposed to close enough. The interface between tissues is (absent prior surgery or other damage) subtle but distinct: soft, easily separable, and comparatively bloodless: it will allow you in and welcome you like the gentlest of innkeepers on a cold night. If in exactly the right place, you can separate things easily, in ways that seem indelicate but are in fact the opposite. A few cell layers can make all the difference. When perfectly positioned, you can use your finger, the back end of a scalpel, the closed tips of scissors, and expose your target in a flash. Off by a bit, you'll need to dissect, probe, stop a bleeder here or there, be a little rough, before you've conquered the intended area. And never know the difference! You can spend a whole career unaware there's another way. The gods of surgery will let you pass; but they won't be singing you through the gate.
I've said before, and I'd say again: doing surgery is not really mysterious: those of us who do it are not extraordinary. People can learn it. But I think some are fortunate enough to have certain cerebral software that allows them to see the operative field more clearly; to understand instinctively how to avoid struggling. Among the good point guards (and mid-fielders! -- but you probably don't like soccer as much as I do), some just seem always to make the right pass at the right time: they see the whole game as it's being played out, know what's about to happen. A coach would say that can't be taught. Some just have it.
To a small extent, surgery and surgeons separate along similar lines. Can I say that I had some, without sounding too self-absorbed? The irony is that it surprised me to find it out. I didn't sense it when I chose to become a surgeon, or even as I was learning it. Like a rosebud, it opened with time. And in other ways, surgery was a poor fit for me: it drove me crazy because I couldn't stand imperfection to any degree: even a keloid scar made me feel like a failure. Every night, I lay awake stewing; I was overly paranoid. But I could do the operative work; that I could do.
I owe a lot to the fact that when I first started practice I was in a semi-lousy situation: a town with way too many surgeons. As the new guy, it took a long time to get a following. On the other hand, for lack of much else to do, I assisted every other surgeon in town, many times. Having trained in an in-bred place (meaning the majority of attendings had trained there) I was well-trained but exposed to a narrow range of techniques and surgical philosophies. In my first practice experience, I saw things I'd not seen before; both good and bad. My operative approach became an amalgamation of ideas I picked up from many sources; and as time passed, I added my own.
Because of Vic, I placed a nearly obsessive premium on efficiency, on considering everything I did from the point of view of whether it made sense -- whether there might be a better way. And over the years, I found some. I won't list them, but I was always either figuring out or stealing little tricks here and there for every operation I did, all for the better. Most surgeons do, I'd add.
So yeah, I was one of the fast ones. Faster, eventually, than Vic himself. Sure, I tie knots ok, but you'd definitely be able to see the fingers without blurring. I admit it: I liked being fast. Hearing people mention it. Appreciation from anesthesia people, scrub nurses. Taking some sick patient to the OR from the ICU, doing something serious, wheeling the gurney back to the Unit myself, hearing the nurses say, "Wow, you're back already?!" Being able to do more surgery in my assigned block of hours than anyone else. (That, of course, has obvious remunerative benefits as well.)
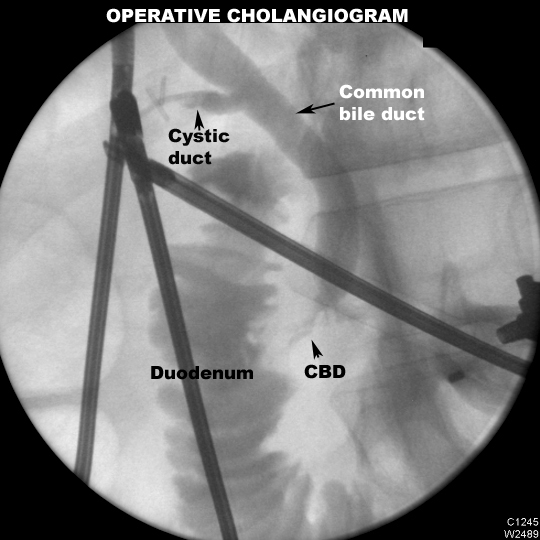
There were times I actually delayed talking to families in the waiting room because I figured they'd either wonder if I took some sort of dangerous shortcut, or decide the operation was so easy I shouldn't be charging for it. One of those times was when I removed a gallbladder, including taking an intra-operative bile-duct Xray (cholangiogram) in twelve minutes. Skin to skin.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}