
They told me in medical school that the diagnosticians of old could thump on a chest and detect a tumor as small as a centimeter. I'm not sure I ever believed it, but I've always had a love for the art of physical diagnosis -- of touching, feeling, listening to the body, and coming to an understanding. As technology invades and pervades, that art is becoming almost (not quite) superfluous and antiquated; an amusing throwback. Look at that old guy, touching his patient. Sweet, really, if a little creepy. Hasn't he heard of ultrasound? Actually, I have. A realist, I've ordered a ton of 'em. Still, I think that more than anything else what makes a doctor a physician is the ability to use the senses to figure out what's going on. It's a wonderful combination of book-learning and the accumulation of experience, of sensory attunement to another person. It's very cool.
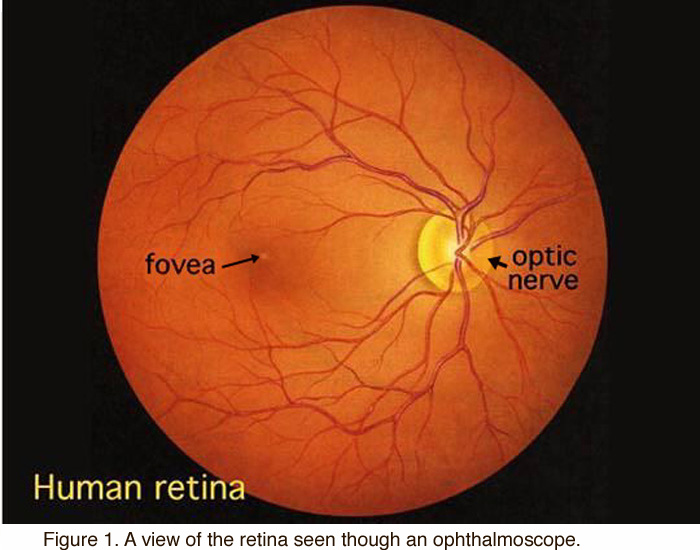
In med school, things are revealed one or two at a time, and each finding seems like a little miracle. I remember sitting across from my roommates, getting the hang of an opthalmoscope, using -- as is necessary -- my left eye to see into their left, my right to their right. Frustrated by the red reflex, finally getting past it to see the eye grounds: the retina with its tell-tale vessels and their disease-revealing crossings of each other. The best of the best: the optic nerve. Thumb the wheel to get focus, get the depth right, and there it is. Breathtaking: now, I'm a doctor. Hearing the split heart sounds? Well, I went into surgery.
If you strum a plastic comb next to your ear, the sound it makes is similar to that of obstructed bowel. When examining for appendicitis, it's best to use one finger: point tenderness -- pain in one spot and less right next to it -- is a tipoff. Those things are textbook stuff, teachable. Gauging the tension of an abdominal wall by touch and percussion, judging the sound of the thump -- that's art, based on assimilated input over a lot of cases. If you want to assess perfusion in shock, feel the knees. Looking for subtle differences in circulation to the feet? Place each hand on a foot, hold them there, then switch: differences in temperature will be doubled. Tricks, picked up on the street. They have ultrasounds to see if your bladder is full, measure the exact number of cc's of urine in it. I can get close enough with a thump and a touch. So could you.
No matter how much data I'd checked ahead of time -- labs, Xrays, chart notes -- I never really got the true sense of things until I saw the patient, touched him or her, listened to their words and the sounds of their bodies. Saw their faces. Smelled the air in the room, or their bandages. And yes: poked my finger into their rear end. To the patient -- who knows? -- perhaps it seems like ritual, like posing. Going through the doctor motions. Or maybe it's mysterious and awesome, like a conjurer, a mystic, a whole-body palmist.
Following a careful history and physical exam, I've taken out appendices without the benefit of an ultrasound or CT scan. Same with gallbladders. Even colons, sometimes. Nowadays it feels a lot like insanity, hanging out there too far. Know what? It is.
Every once in a while I'd catch myself, still with my hand on a belly while sitting on the bed talking to the patient and family about my impression, my recommendations. Long-since having garnered the information to be had from palpation, I somehow liked to maintain that touch. As inspiring as it is to be allowed to operate, literally to enter into a bond and to breach boundaries of flesh that only a few are privileged to do, the physical exam has a special intimacy of its own. A unique moment of connection with a fellow being heightened by practical knowledge and distilled experience, it's way more than ritual and show and it ought never to be fully supplanted by magnets and beams. Drawing on all the senses, and the ability to synthesize them; bringing together knowledge, skill, and instinct, as human as it gets, the exam depends on who we are and what we're made of. There's really nothing like it.




{kind=link}
{kind=link}
{kind=link}
9 comments:
Great post, as always, Doc (I missed Car Talk today, but see if I can hear an archived copy to see if you made it on!)
I'm in my first year of surgery residency, and am somewhat conflicted - I absolutely love the idea of having better physical exam skills, but when you're busy (and what intern ever isn't) it's just so much easier to order a test or study to "rule in or rule out" a particular diagnosis (such an odd turn of phrase - maybe a subject for a future post of yours?).
Plus, the liability. Will today's climate accept the oft-quoted "10%" false positive rate for clinically-diagnosed appendicitis? I still see people go to the OR without scans these days, the "slam-dunk" ones clinically, but I'm always (pleasantly) surprised... and I always make sure to ask what the appendix looked like when they got in.
My program has just about mandated that all central lines be done with ultrasound.... not because they doubt our abilities, but because JCAHO is almost mandating it (although, in all honesty, it would have prevented a poor guy last year from getting a carotid cannulated...
Anyway, there are a few esteemed graybeards left in my program that heavily push PE skills, and woe to the resident who can't describe the findings, so we are left to heavily mine their experience, despite realizing that we will most likely never achieve the same level of physical exam acumen... (I dare say you know and have trained with some of them, being in the same part of the country).
Great post, as always, Doc!
Neurologists are in a bit of the same thing as well. When I was in med school was when the first CT scans came out, in my residency, MRIs.
There are certainly many heated discussions I recall in the early days of scanning about the significance of findings on neurologic exam, only to be disproven by the scan.
At the same time, listening to a neuroradiologist talk about what they think is going on with the patient can be humorous -- the imaging info is not very useful without the clinical connection.
I am a Massage therapist that got here through a Google alert. Besides the palpation training in school I worked for a chiropractor that had a system for recording palpation on the client chart. At first I just recorded his findings as he called them out but eventualy on routine clients I was expected to do the periodic exam. I also got to take and mesure the x-ray film. So I developed a corilation between what I was fealing and what I saw. after 12 years I have become very adept at seeing with my hands ad feeling with my eyes.
Hans Albert Quistorff, LMP
Antalgic Posture Pain Specialist
So, radiology or thumping? One is expensive, one isn't.
Does it just come down to reliability?
I appreciate when a doctor spends the time to do a physical exam. I've usually been able to point out details of my problem, and ask questions, that wouldn't be possible if the doctor just says something like "I'm sending you for a CAT scan." I also feel that the doctor has more concrete information about me and my problem when he/she has done an exam.
I don't have similarly positive feelings when I have had a sleepy, harried resident do a physical exam, as if it's an onerous chore to be gotten through as quickly as possible. Which, I gather, is exactly what they are being trained to think.
Who needs a chest X-ray if you can demonstrate whispering pectoriloquy?
(Nice name for a yacht...)
Try
Orient, JM: Sapira's Art & science of bedside diagnosis, 3e. 2005
DeGowin, Swartz, Bates & Sidel's books are the most simple & recommended physical diag bks.
PocketRadiologist has a nice little series
and Silen: Cope's Early Diag Actue Abdomen is always interesting
"As inspiring as it is to be allowed to operate, literally to enter into a bond and to breach boundaries of flesh that only a few are privileged to do, the physical exam has a special intimacy of its own."
So eloquently said. Good post! :)
Amen x3.
"I've taken out appendices without the benefit of an ultrasound or CT scan...Nowadays it feels a lot like insanity, hanging out there too far."
I simply consider that as being a doctor--a diagnostician being just part of that title--not just a "cutter." All the technology is a confirmation, not a subtitute, for the diagnosis.
Regarding the retina, I too remember the thrill last year of finally finding the optic disc amidst serpentine projections of various unnamed vessels. I was so excited! That was dampened quickly when my classmate, who had to sit patiently for an unnatural amount of time with a 5 gigawatt light in his eye said, "I hope my blindess was worth it." heh.
Post a Comment