
I've only had to do one emergency tracheostomy, and it was scary. On the other hand, I've done many a trach (pronounced "trake") less emergently, and it can still be a little frightening, even on a pink patient. Not to mention the potential for turning into a circus.
I view it as community service. Taking only a few minutes of operative time and reimbursed as if it took even less, the whole rigmarole potentially requires all sorts of extra, non-operative, effort. In the typical situation, the patient is in the intensive care unit, mechanically ventilated via an endotracheal tube passing either through the nose or mouth. At some point the tube becomes intolerably uncomfortable and/or potentially damaging to the tissues through which it passes. In addition, it's hard to suction properly (which is necessary because such patients can't cough stuff up on their own) through such a long pipe. So the surgeon is called to switch the patient over to a tracheostomy. It's more comfortable and allows easier hygiene and airway maintenance. [Aside: there's nothing more annoying than getting the "request" via an order written in the chart by the attending physician saying, "On call surgeon to perform tracheostomy." Like ordering a blood test; how inexcusably rude!! It always pissed me off. Depending on my mood and how well I knew the nurse calling me (some quite understood), I might respond that if Dr Soandso wishes me to see his patient, he can damn well call me and say so. Or I'd just grumble in my gut and go do it.]
Often the patient is unable to sign for or understand the procedure. The family needs tracking down, meetings set up. Transporting a patient on a ventilator -- with a fertile bloom of accompanying other tubes and monitors, several IVs, compression boots, precarious arterial lines -- to the operating room requires coordination with respiratory therapy and/or anesthesia, arranging for a couple of nurses to accompany, and to time it such that the patient travels straight from the ICU to the actual operating room, with no stop in a holding area. It's usually a fairly well worked-out process; still, there are risks and worries. In any case, in terms of time, hassle and worry versus reward, there's not much in it for me. Community service, as I said.
In training, on the cardiac service, we did our trachs in the ICU, under local, with a scrub nurse from the OR, a full instrument pack, a portable operating light, and with an anesthesiologist present as well. The belief was that potential risk of doing it outside the OR was balanced by eliminating the hazards of travel. I'm ambivalent about that, but it was good practice. I learned to do it with a very small incision, and in what I think is a very safe way. Nevertheless, in all the hospitals at which I practiced after training, ICU trachs weren't allowed. They all had stories...
The operation can usually be done though a small incision, one that hides behind the "shield" part of the tracheostomy tube. There are a few tricks, starting with proper positioning. Doing it while the patient remains in the hospital bed is possible, but unpleasant. Because of the width, you have to lean over too far, and it makes the back of the knees hurt like hell. Transferring to the OR table, though, presents a risky moment or two, potentially dislodging this or that, but is, probably, preferable. Either way, rolls of some sort are placed behind the lower neck or upper back so the neck is extended. Sometimes it doesn't help much: people with thick and short necks can be a nightmare, as can those with big thyroids. Conversely, those with necks like a swan, lithe and lanky and thin and graceful, landmarks visible across the room, are worth the logistical struggle just for the pleasure...
The three most important technical issues are these: 1) after making the incision, dissect exactly in the midline (thin=easy; thick=not so much), spreading Metzenbaum scissors vertically only, all the way down to the trachea; 2) use Army-Navy retractors in the wound as it's deepened, one on each side, pulling laterally, to expose; and 3) when the proper location (the first tracheal ring) has been exposed, place fat silk (or any other non-absorbable and soft) sutures, one on either side of the midline of the cartilage, before incising the ring. They make great handles for traction when inserting the tube, and leaving them for a few days facilitates replacement if necessary. Especially if needed in a hurry.
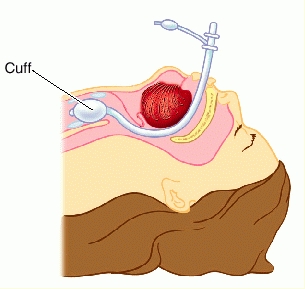
The meat of the operation is the actual insertion of the tube. It's a dance with the anesthesia person: after incising the trachea and lifting on the sutures, you watch closely as the person at the head of the table slowly pulls the endotracheal tube back, until the tip of it is just above your incision. At this point, the patient is no longer being ventilated, because the air/gas being squeezed in is rushing out the hole in the trachea (you smell it; environmental rules are suspended). Sometimes there's coughing, and mucus blowing out the hole. Because of the forward curve of the trach tube, and of the backward curve of the trachea itself, the tube must be inserted sideways and then twisted and plunged downward -- without tearing the balloon on the cut edge of tracheal ring. Depending on the respiratory needs of the patient, this moment can be tense. Rarely, you need to regroup and have the anesthetist re-advance the existing tube. But once the trach is seated, which is usually very quick and smooth, it's all over. No need for suturing (assuming you made the incision properly small); just receive the ventilator hose from the anesthetist, plug it onto the tracheostomy tube and exhale, tension dissipated like breath in a cold breeze. Then tie it in place with twill tape around the neck, and call it a day. Except for wheeling the patient back to the ICU, explaining to the nurse why those sutures are hanging out, and telling the family that everything is okay.
[For a couple of harrowing tracheostomy tales, with diametrical outcomes, the reader is humbly referred to my book.]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
13 comments:
This is a wonderful description, and it makes for great patient teaching, too. Have you ever encountered sub-Q emphysema? In the days of the first AIDS patients(pre-the known diagnosis) blowing their lungs and having tremendous PEEPs, I encountered a fair number of patients who suffered from this. Nothing like that bubble wrap crackle to get people's attention!
Those were also the days of single glove suctioning, where the exposed hand often developed infactions from the open tot he patient suction control valve....
I agree with Annie. Your description is wonderful and clear.
Sorry, comment re-worked due to poor spell-checking on my part.
At the last hospital that I worked, ICU trachs were common. They were done by the surgeon and pulmonologist with the respiratory therapist and ICU nurse assisting.
Good post. I ALWAYS perform a trach with a tight sphincter. Airway, baby. Don't lose it. I prefer the OR for these, just because of lighting and it's a pain in the ass to have the right instruments delivered to the ICU.
Any thoughts on the percutaneous trachs? They always seemed needlessly dangerous to me.
Buckeye: I never tried one. I could imagine a situation in an ER where it would be a useful option to have available...
Are there cases outside the hospital where an emergency trach would be done a la MacGyver by using a Boy Scout knife and the tube of a pen?
Yes!
When I was a rotating intern at Charity Hospital in New Orleans, part of the standard orders for a kid with epiglotitis was to have a trach set at the bedside. That gave me nightmares, to think about being called up to actually use it. I had seen it done and knew the principles but never did one. Thank God I never had to try. I was pretty happy when the idea came up to put a 14 ga needle in the cricoid as emergency ventilation. I never did that either but thinking about it didnt give me the same heebie-jeebies.
Good post -- I've done 3 emerg trach's. One just a couple of weeks ago holding the sticks for the ENT (thank goodness) -- still hit a bleeder (which I momentarily thought was the subclavian) and s*** my pants. One on a ward (couldn't get the tube in on time) and one in the dead of night on an emerg pt with a squamous cell blocking the airway. I was so tired (babysitting someone in CHF all night) that I saw an RT run down the hallway with a flex bronchoscope and thought "ha -- who's the poor bastard that has to manage that airway disaster at 4am" only to get paged two seconds later. There's too many important pieces of anatomy in the area -- more than happy to have ENT involved.
I do essentially all of my trachs percutaneously, but learned the standard way in residency.
It still get's me a bit anxious.
I'd say that unfortunately, this and many other "basic" general surgery procedures are included in my "not really worth doing" list.
I'd include PEG's (have one tomorrow), ports, and lines in that list.
We do all our trachs percutaneously. We have a relatively busy Trauma service at our Level 2 center and our standard practice is an ICU bedside trach with one of us doing the perc trach (Cook Blue Rhino kit) and another with a fiberoptic bronchoscope. Nurse and Respiratory Therapy in attendance as well.
No real anxiety and it's over in 5 minutes.
I thoroughly enjoyed this post. In PICU we do the occasional perc trach at the bedside, but most are done in theatre which thankfully is a very easy trip through the doors at the end of the unit.
I often think of the contrast between ENT surgeons where I work, one who manages very small neat incisions that produce an extremely stable airway, and one who unfortunately seems to prefer a 'gaping' approach. I have a great deal of sympathy for these guys given the difficulty of the procedure, particularly in children, but it really does make management much more difficult with a large wound.
Post a Comment