
What to do with a patient referred for a finding that you can't interpret on a test you'd never have ordered? It's a tough one, and not as rare as you might think, especially in the area of breast lumps. As a topic for posting, the subject comes up in a roundabout way. A couple of other medical bloggers picked up on my mammorable patient" post, and a comment on Orac's site raised the issue of the morbidity of medical screening. It's a fruitful object of scrutiny: false positives, for example, (a finding that requires further evaluation, possibly invasively, that turns out to be nothing) add up on the other side of the ledger. If a person suffers harm -- or even death -- from investigation arising from some sort of routine screening (for whatever...), when the issue raised turns out to be harmless, well, that's not a good thing. There's lots to say about it. I won't, exactly, now. It's just that it reminded me of something that used to drive me crazy.
I could rant all day and into the night about evaluation of breast lumps and where I think the surgeon's role ought to begin. I had a sometimes friendly, sometimes antagonistic relationship with a number of radiologists over breast evaluation, and I tried over my whole career to educate (based on my own biases, of course) primary care docs in the matter of breast lumps. A dispassionate review would likely show I won the occasional battle, but lost the war.
In a nutshell, it comes down to this: when there's a lump you can feel, diagnostic imaging (Xrays, ultrasound, etc.) is a waste of time and money. OK, that's a bit over the top: you get needed information about the rest of the breast, and the other side, which will come into play at some point. But getting a bunch of studies -- particularly without the input of a surgeon -- as the initial step in working up a lump adds up to lots of unnecessary running around for the patient, distractions in the diagnostic process, and -- not rarely -- detours into side roads that never needed taking. Ain't nothing like a good physical exam by a person highly familiar with breast exams, followed, when indicated, by the quick poke of a needle. Don't get me wrong. I recognize that radiologists do good in this world. In fact, I'll admit that the occasional interventional radiologist has saved my bacon more than once, with a well-aimed drain into an abscess here or there. But as the evaluators of a palpable lump (emphasis: palpable. When you can't feel it, that's a whole different ball of wax), they either muddy or bloody the waters.
Mild to moderate disclaimer: ultrasound quality and interpretation is constantly improving. It probably has a role in the screening of breasts too dense for useful mammographic interpretation; and as specificity improves, it may become more reliable in the interpretation of solid lesions. But, basically, the value of ultrasound in the study of the breast is to determine if a thing is solid (which means a possible tumor in need of a biopsy, usually) or liquid (which means, almost always, a harmless cyst in need of no further investigation.) And when is it useful? When a thing shows on a mammogram, and when the thing can't be felt. Period. If you can feel the thing, poking a needle into it gives the same info and more; cheaper, quicker, and more definitive. If it's a cyst, the needle will produce fluid and can empty the cavity, which in most cases makes it go away permanently. So it's diagnostic and therapeutic. Or if the thing is solid, then with the knowledge of simple technique, a sample can be taken with the needle, smeared on a slide, and reviewed under the microscope; often giving a final answer. It makes me lunatic bonkers when the first stop for a woman with a lump is the radiologist's store.
She finds a lump in her breast: it's round, tender, and she's sure it wasn't there a month ago. Because it's the way things work, she sees her primary doc who -- because it's the way things work -- sends her for an ultrasound. Or, more likely, a mammogram and ultrasound. Or a mammogram, leading to an ultrasound which is hopefully done at the same time, but maybe requires a return visit. As expected, the finding is of a fluid-filled cavity consistent with a cyst. (Once in a while, the report will refer to some "debris" floating in the liquid, or some echoes that suggest some irregularity in the cyst wall, of uncertain significance. Now she's worried. My office gets a call: our patient is scared to death over her report. Can you work her in today? Even if there's not the fear element, she's coming to see me much later and lighter in the wallet than if I'd gotten a call about it in the first instance. So I see her, use my handy little needle, diagnose and disappear the cyst, talk to her about cystic breast problems. Depending on age, time since last one, I might have ordered a mammogram, if I'd seen her first. (There's another reason for holding off on it: why get a picture of a thing that'll be gone?)
But it gets more complicated: she gets her ultrasound, and it shows a simple harmless cyst, as expected. But of course the whole breast has been scanned, and wouldn't you know they saw a five millimeter (less than a quarter of an inch) something somewhere else, too small to characterize fully, can't rule out every bad thing on the planet. See, that's what I was talking about. What to do with something you can't interpret on a test you wouldn't have ordered, found in an area not even part of the original concern? Just to make it realistic -- and worse -- the radiologist who read the study has recommended ultrasound-guided biopsy of this tiny spot.
What I'd do is candidly tell the woman my feelings on the matter: that I think ultrasound is the least reliable and reproducible of the studies we do on a breast; that I'd not have ordered that test in this situation, and that whatever this incidental finding is, at that size it's most likely perfectly safe to leave it alone for now and repeat the test in a couple of months. And that based on my experience, if repeated in that time-frame, it's quite likely it will no longer be there. And, of course, I'd also explain that there's no way to be sure at this point and that if it'd drive her crazy to wait, we should arrange for a biopsy. (In several of such cases, the scheduled procedure was unsuccessful in finding the original lesion.)
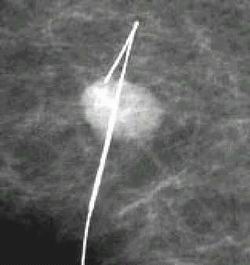
In the case of large lumps in the breast, I've seen women sent for mammogram and then, per recommendation of the radiologist, undergo stereotactic biopsy. That procedure is intended for things seen on mammogram and not feelable: whether the recommendation was based on an unskilled exam or without an exam at all, it's an expensive and cumbersome way to handle tissue sampling when a simple office aspiration would have gotten the same info. I've seen infections from such biopsies which the radiologist feels uncomfortable in handling; so I see the patient ex post facto, having received an unnecessary procedure and now, salt in the wound, I'm to care for the complication.
What's the point here? Not, despite appearances, to say that radiologists are the enemy. Rather, it's to say that with breast problems more than any "surgical" problem I can think of, coordination of care makes for better care; more economical, more efficient, less stressful. At worst, it can be fragmented into disconnected pieces, where doctors see the problem through a narrow lens, applying tools at their disposal no matter the alternatives. At best, it can come together in a true breast care center, dedicated to comprehensive and complete care. In the best of all possible worlds, surgeons, radiologists, pathologists, and oncologists are under the same roof and consult freely before diagnostic and therapeutic decisions are made. Such centers exist. They're not widespread; and, sad to say, there are some bogus outfits out there. I know of so-called "women's breast care centers" that imply broad-based care but which in reality are drop-in centers that encourage women to show up without referral, to have a cursory exam, mammogram, and quite often an unnecessary ultrasound. The results, rather than explained and followed up upon, are handed to the woman with instructions to see her doctor. It's a rip-off, not run by legitimate radiologists with honorable intentions, but by guys out to make a buck; some aren't even fully certified radiologists.
In most communities, women with breast problems have to start with their primary doc, and then follow a circuitous path to diagnosis and treatment. The end result is going to be good care, but it's hardly the most efficient journey. It's a microcosm of American healthcare: limited by the absence of agreed-upon protocols, complicated by varying levels of expertise, sullied sometimes by docs guided by self-interest (or at least a limited view), marked by wide variations in efficiencies and cooperation. And it showcases a central unclarity: is the best care delivered via good ol' Doc Jones, who knows and cares for the whole patient, or by taking certain body parts containing certain problems to a specialty center right off the bat? I guess if every doc in every area of practice were perfect, and had skills and knowledge equal to every other doc in their field, the question would be moot.


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}